
- Pharma Costs of market approach in control
- From pharma mass detailing to Key Customer Focus
- Focus as key to pharma success
- Intervention points to create a focused commercial cycle for pharma
- What tools to use to detail the pharma commercial cycle
A chalkboard scheme to sketch the new pharma market approach
Following up the presentation of our project with a pharma company in the Netherlands on How Pharma can enhance its impact and reduce costs of marketing, we present our chalkboard sketch to construe a new commercial model for a pharmaceutical market approach.
In review of our success we began to reflect and study the basic issues of our approach: an approach that would guide the decision makers in the company to construe the right set of activities to focus on accounts with the best chances of success, engage with its decision makers on drug prescription effectively and provide added value to their medicines so as to help care providers to help their patients better.
Strategic departure

The model starts with the acknowledgement that there is not one right way for approaching all different markets to pharma with a standard approach. Preference schemes for drug selection, local protocols, reimbursement schemes, actual health care systems’ conditions, drug prices, different stakeholders and the very portfolio of the company, can only lead to the conclusion that differentiation should be the name of the game. (see here). The model needs to accommodate for these different conditions.
We will also depart from the acknowledgement that the company’s choice for its market position might be on either one of both ends of the strategic dimension for pharmaceutical companies: ¨towards the position of being a producer of (generic) drugs, not relating to its use and application in therapies (other than just the method of administering the medicine), or to the opposite side, as in being a partner to the provision of health care instead.
To a generic producer of drugs, more and more markets seem to give only temporarily opportunity to sell and deliver (generic) drugs at a relatively low price, until there is a new supplier that has to its advantage a still cheaper price and/or a USP in its supply chain. No wonder that classic generic companies turn to branded generics to avoid the commodity trap.
As a partner in health care instead, the company might choose to work together with care providers and patients to figure out and develop, or even co-create best practices for therapy, integrate all aspects of the care process, like informing patients, help to co-create care paths, give support to the practice of shared decision making, instruction and guidance in therapy, foster on and offline communication regarding questions by patients, facilitate communication between care providers, adjust therapy in care of daily monitoring data, etc. It is no doubt that because of its drug research and development activities, pharma has several sorts of expertise and data that will contribute to care of patients. In the frame of developing personal medicine, more of this can be expected, and pharma should get ready for that.
By the ongoing development in emerging, mature and advanced markets, pharma will be challenged to the sustainability of its role to health care. It might even need to choose between either creation of new drugs or marketing and supply of medication to care providers and patients. Is one company capable enough for both the creation and marketing of drugs and be able to lead these to effective results?
Yet, the new commercial model to pharma’s market approach needs to accommodate for both strategic intentions. A positive development of the pharma company to either role is related to characteristics of the disease and preconditions of specific markets: regulations, reimbursement schemes and buyer systems, but also drug therapies, local conditions of care provision and contexts of care to patients, etc. ¨In any case, the roadmap for pharma’s development of its role in care will be divers: inspired by actual strategy, diseases covered, its portfolio, general (country and/or area bounded) market conditions and local contexts.” ¹
Intention
It is the intention of the model to guide the pharma decision maker to an optimal market approach for specific market conditions, to bridge strategic global intentions to local performance activities and to define the actions to realize pharmaceutical intentions in specific market contexts and health care system developments. ¨By now, every pharmaceutical company has come to acknowledge the large differences between regional markets, between countries, and also, between regions within countries, like in Spain and France in Europe, and like differences in urban and rural regions in Russia. Moreover, different paces in healthcare system developments within a country will give rise to changing local characteristics of care, be it different patterns of cooperation between care providers, the ICT systems in use, medical protocols and diverse arrangements in actual care processes. It is right isn’t it, that despite all standards of medical protocols, the actual care given is different. And still, at this point, I don’t speak yet about differences in perception and personal experiences of patients.
The model needs to enable different implementation tactics and activities, effective and efficient in its proper contexts. As local care characteristics and Rx conditions differ, specific approaches need to be defined in line with these and must enable developments from that point onwards. Effectiveness of standard detailing in promotion will only (still) be optimal in certain niche markets and will turn out to be bluntly ineffective when adopted as the dominant market promotion tool everywhere.
The model will also suggest use of new market approaches, like on-line information, education activities, social media, mobile applications, multichannel management, and data registering routines through ICT support systems. It will also suggest directions for its features, data and outcomes. Current programs like CRM, CLM, market access, KAM, Customer excellence, multichannel management and other ideas packed in modern pharmaceutical industry’s sales and marketing procedures, might so be aligned to build meaningful information to their users, instead of presenting a vast but fragmented overload of data.
The model will guide the decision maker to effective use when deemed feasible and appropriate in contexts of specific and different markets.
What are the criteria for the new commercial model of pharma?
In short:
- Pragmatic functionality: helping to bridge strategic global intentions to regional and local tactics – to enable specific developments into practical hands on activities. For effectiveness and efficiency, i.e. ROI, an integrated view on all different market and customer related activity, is a prerequisite: an integrated view from market access on to service activities. It also implies a multidisciplinary cooperation within the organisation. Aligning internal silos;
- Differentiation upon external conditions to the business, both global, regional and local: from governing market regulations and rulings to local care and treatment conditions; and from emerging health care system varieties to market approach constraints in advanced markets;
- Differentiation to internal routines from marketing to medical and sales to (lack of) desired new competencies to all customer facing forces: from standardized classic individual promotion to account based development and support plans;
- Adaptability to local conditions for Rx. Segmentation of accounts. Not just in potential of quantity of patients with defined disease conditions, but in quality characteristics of care provided too. This enables focus on accounts in terms of chances of success of a proper proposition, instead of a pursuit of unattainable potential;
- A development perspective to suggest opportunities to intensify company – customer – patients relations so as to create benefits of these relations to outcomes of care and to (material and immaterial) profits for all related stakeholders and protagonists in care;
- Specific suggestions to the use of concrete tactics and tools under specified conditions facilitating targets of engagement, involvement and (co-creative) development.
- Indication of ICT support systems and/or identification of instruments/tools to the development of professionals of the pharma company to get along with these developments and create challenge and motivation to do so.


The draft of the pharma commercial model
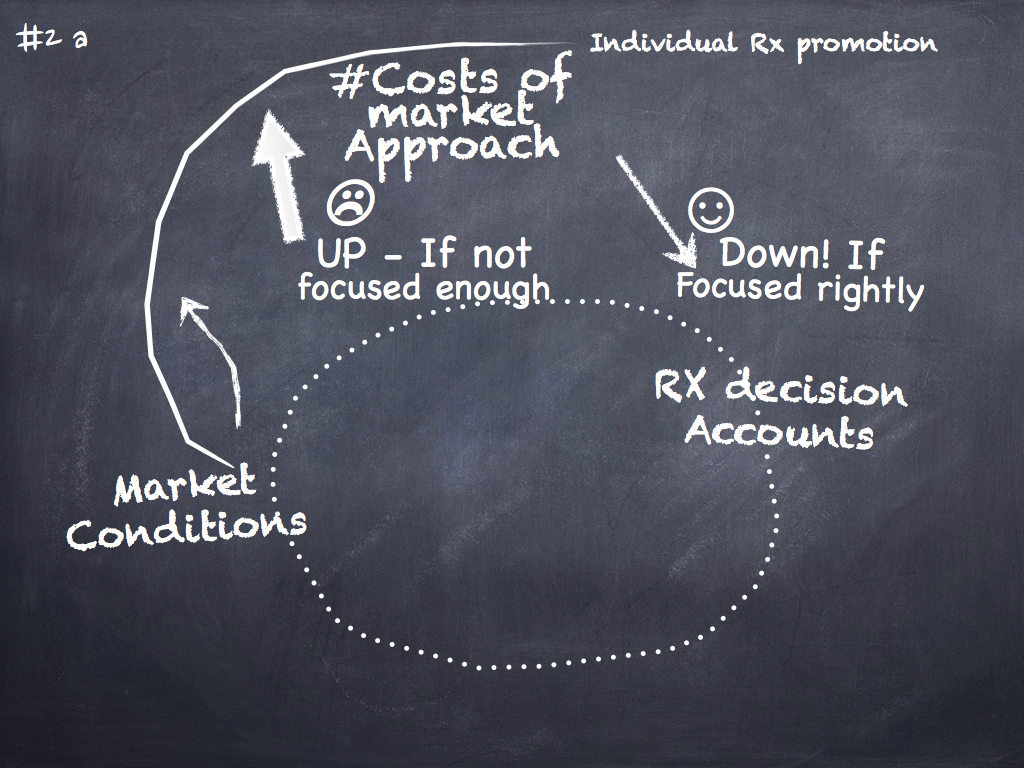
With these criteria in mind, we started the transformation of our experiences into a preliminary sketch of the pharma commercial model with a general draft of the commercial cycle. See board #1.
The core elements that define the market need to lead the market approach: starting from profiling the market conditions at the one side, on to selection and engagement with customers/accounts at the other. In this draft it is easy to depict how standard detailing, even to potential customers, would turn out raising costs with doubtful return, whereas increased focus on defined and selected customers would decline costs and raise benefits.
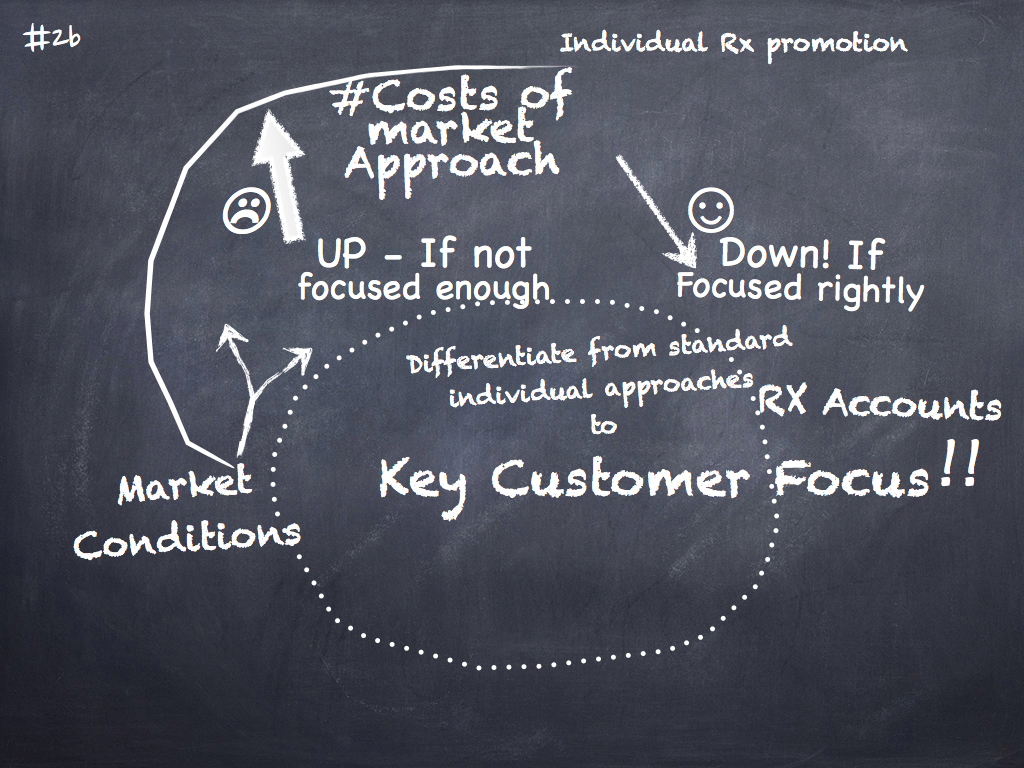
Focus priority
As you can see in the blackboard sketch, standard detailing to doctors moves away from specific engagement with Rx decision makers in networks around them, whereas focused approaches can pick up on specific information coming from account profiles.² 
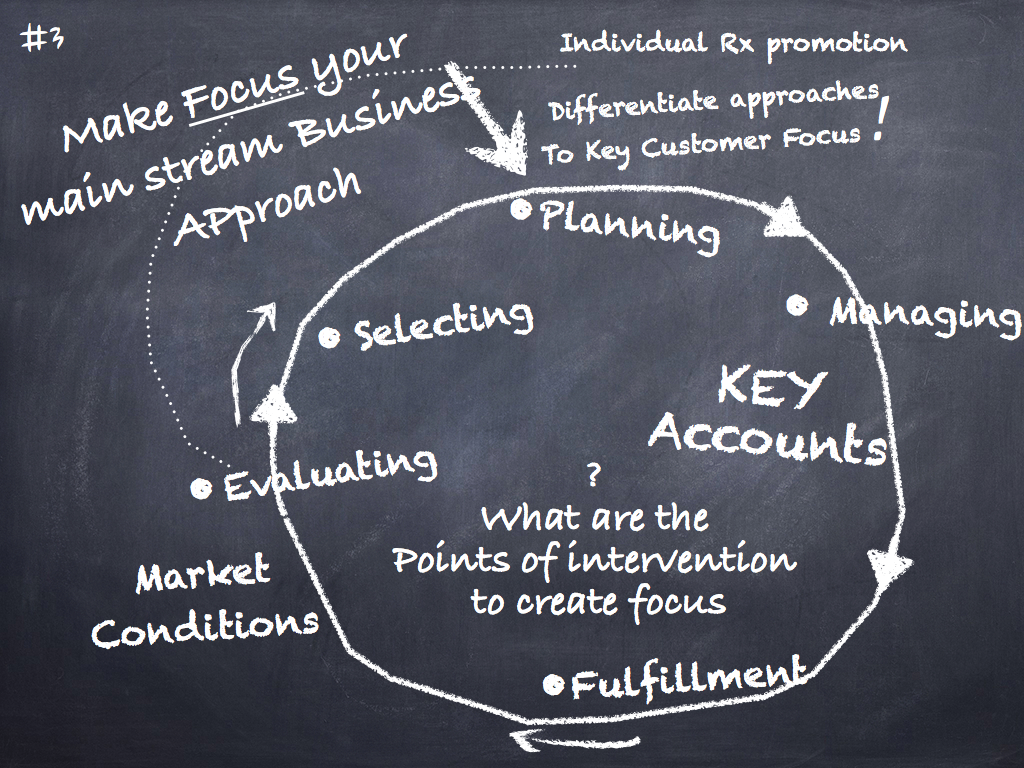
Focus: the main stream business approach?
One can define focus in terms of several dimensions and intentions. Focus is the instrument to tune in to the conditions the market presents to the business. Actual focus is made up by a cycle of analysis, evaluating, selecting, planning, management and fulfillment, turning into evaluation again. See board #3.
This is not only necessary to establish the results of actions, but also to keep track of changes in market conditions that occur along the way. In the Netherlands, we have had to perform two cycles of these per year due to the dynamic nature of the transformation phase of the Dutch health care system. Also, because of this, we rather created quick feedback to see how our marketing efforts showed results in the desired direction. But, to enable one to “see†the sometimes really subtle effects, one needs to know where to look at.
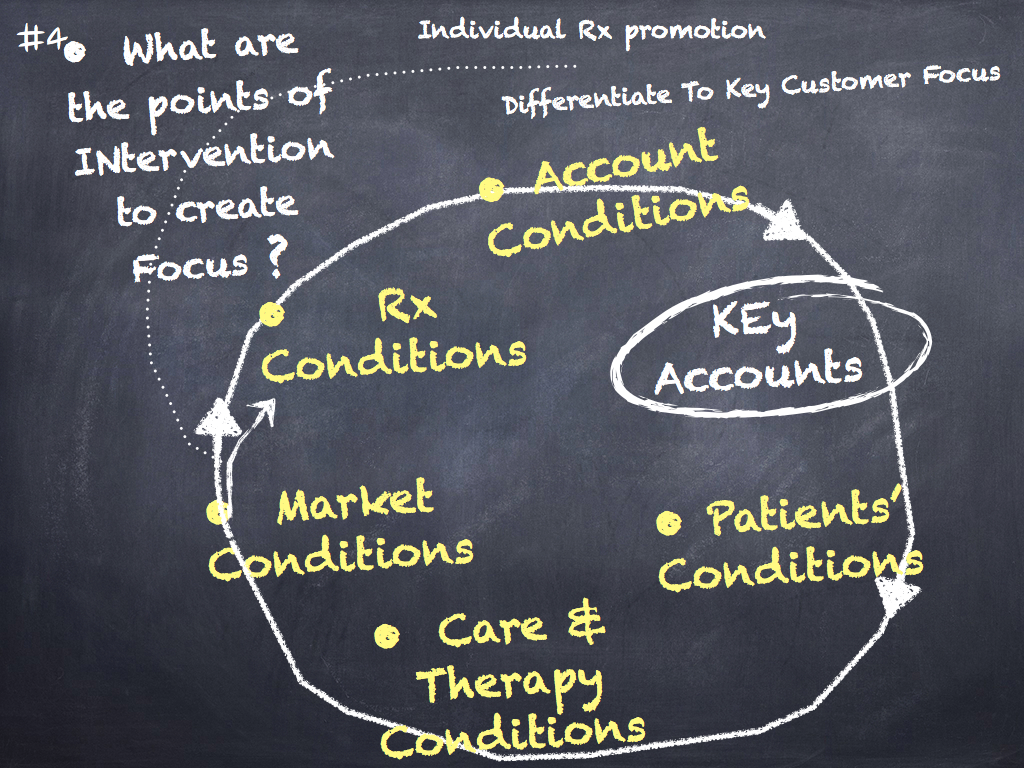
What are the points of intervention to create focus?
Segmentation and targeting of accounts for the market approach is usually done exclusively on individual physicians’ potential, ever since the publication of McKinsey’s “Making more of pharma’s sales forces” (2002); for certain an important variable to know one’s customer, but surely not the only one. See board #4.
When a pharma company wants to play an active role to support medication in care, to add real value to its therapy, these are the variables to adapt to: general market conditions, Rx, reimbursement and account conditions, but surely too conditions related with patients, their care and therapy.
Systems’ differences between several types of care, like emergency care, hospital, chronic, family, longterm and elderly care, create contexts of medication that will impact the use and effects of therapy. These will for instance influence the relatively early discontinuation of taking medicines by patients. Mind the actual interest for therapy compliance, where one looks to remind patients of their medication, whereas the experiences of issues intervening individual compliance will be more than just that. The evolving use of national, regional and local protocols is a convincing example too. It means that for decisions regarding the market approach, one would like at least to check these conditions that might seriously influence the selection, prescription and use of medication. Furthermore, one needs to know these varying conditions not only as for their influence on medication decisions, but also to analyze them on opportunities to create support for care that might also improve the use of one’s proper medications. In our experiences, just going through them, to inspect opportunities for service, often results in surprised reactions like: “..that we did not see this before!”
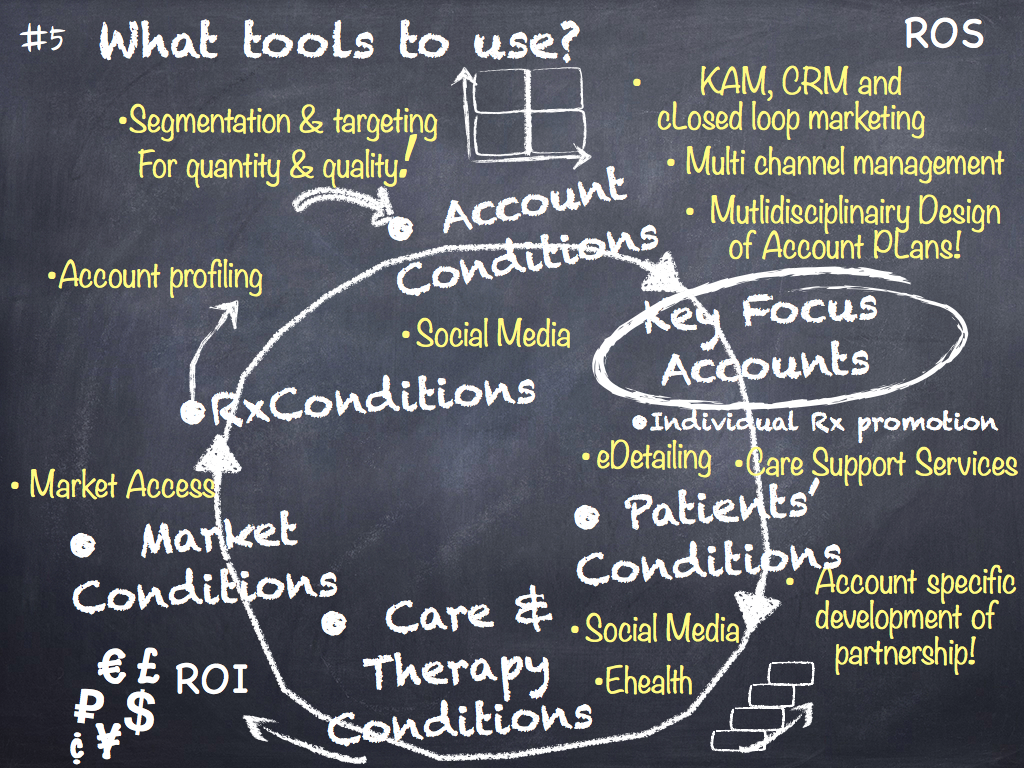
What tools to use?
One needs to know how to convert these starting points into hands on activities. In Board #5 we specify the commonly known programs to market approach that are currently used by pharma companies. However, as any program has some promise of a better reach out to customers, the question is whether a sum of al these do bring about more effect. As a decision maker, you want to prohibit ineffective (current) routines to continue. In fact, one wants to free internal resources for change into a desired direction.
Here, we take every program in fact as a dimension on which a decision to focus can either be defined towards desired activities, or better be left aside. Going through a process of developing and building the configuration of market activities cycle by cycle, we were able to decide every year about the growth of account focused activities, in line with the company’s strategy. We did so on grounds of commercial effectiveness, for the definition and development of support activities and to limit detailing activities to an optimum of impact to leave out those that would have nearly no chance whatsoever of success. Every time the demand to increase focus and intensify the engagement with customer accounts, did bring about new activities in the market approach. Because of the recurrent cycles of review and planning we were able to design the configuration activities in an integrative sense, so as to build on effectiveness.
Examples of variety in use of market approach programs
Specific market conditions will indicate varied response opportunities on which to decide about extension or focus of market approach programs. The following examples give some insight into how one may reflect on market conditions and evaluate the programs that are used to create the business. It would demand too much space here to go through them extensively. Further on we turn to the new tools that we had to develop to accommodate our demands for information and action to create customer focus for better care and return of business in specific market contexts.
- Upon knowledge of concrete market conditions, one knows whether market access activities need to focus on national institutes and representatives or would rather need an extension into local activities, e.g. to local protocol committees. Market approaches surely will differ when one’s drug is selected as first of choice, or is attributed with “only when others fail. Specific policies of government and health institutions are very relevant, of course. But, we have seen instances where closer inspection revealed policies not noted earlier by local management: “it had not been asked by international.. “;
- Segmentation and targeting routines. When accounts are targeted based on estimates of potential, one runs the risk of engaging with accounts of actual low chances of success. Such would be obvious when an account is preoccupied in intensive cooperation with a project from a pharma competitor. This information would have come forward if the right qualitative questions would have been asked in the investigation of account profiles. Based on these, we have made a shift in focus, from accounts with hardly any chance of success, to the ones with a green entrance to helping them, like in: .. if we only would have known that before.¨ If sales forces are not asked the right questions, one does not get answers to them because they would not know where to look for;
- Account conditions are also about the characteristics of the relationship with the pharmaceutical company. Never have we seen a more delusory variable in evaluating market characteristics as ‘relationship’: always vastly overrated. Only when one would ask sales about related effective actions, then their estimates of lenient relationships will become reliable. Furthermore, a specific idea of stages of development for the process of relationship building is a precondition. The sales account ladders in which these are often depicted, will not suffice for this, as they are mostly not well defined: nor to concrete conditions to check if a stage is ‘on’ or not, nor elaborated as to what barriers to cross and specifically how then, to arrive at cooperation or even partnership with an account;
- Elsewhere, we have exemplified the role of social media in the development of account relations.
See here and here .
- Edetailing is also a program of promotion that is often not rightly understood in its potential. That will lead to detailing on tablet(computers) in the same manner as on carbon paper, not using its potential to intensify engagement and relationship. Without the right understanding and design of this instrument, one will throw away investments. It might even lead to objected use on the part of physicians, leading to closed doors whereas the opposite was a promise.
- Multichannel management as an upcoming phenomenon in pharmaceutical marketing is mostly exemplified in terms of how to control several channels in promotion, e.g. in terms of what the right balance of using them would be to campaigns. Instead, multichannel management needs to specify the pattern of interactive relationships, the very lines of communication with customers! This will prevent chaos on the part of the customer in knowing how to relate to the company, i.e. how to reach a specific person with a specific question or demand. Actual lay-out of communication and workflow to inform accounts, of support activities and of defined project activities, might help to (re)design communication patterns to facilitate quick and effective interaction with customers;
- Although conditions of therapy, of care routines and patients, are mostly in the attention of marketing and not so much of sales, their cooperation to investigate both general trends and localized conditions, will enable to generate just those support services that makes working with the company worthwhile. And even so, implementation of support services at accounts’ sites needs specific insights into local conditions. You might have, with me, the experience of how great projects fall short of implementation, just because the physicians don’t have the spare time to look at them;
- Multidisciplinary work between different departments in pharma companies is difficult. No doubt that it looks multidisciplinary just because all disciplines come to the table, e.g. as in brand team meetings. But actual decision making often appears to be more related to hierarchical structures of the group then to a multidisciplinary accord. Methods of professional design thinking³, prove to help to appreciate actual data and information from accounts and to prevent a fall back into hierarchical communication. They prove to enable to find paths of creativity to work themselves to unthought of solutions and to avoid pitfalls in account development: surely basic conditions to effective account management;

What new tools?
In line with the development of the new approach, we needed to develop several tools, that were not available before. These were developed successfully:
- A market quick scan.
Every marketing/sales cycle needs to begin with a quick and effective update of health care development policies from the major health institutions that will regulate or influence actions by care providers. No need for large research efforts, but quick and reliable schemes for inventory. Any actions in the market that will work contradictory to these, will fall short of effect. Positively however, building upon these, will enable quick wins of one’s actions in the same direction. We developed aimed directions to internal staff and management to give focused and demanded information about the market. We also initiated a national health affairs team to be closely related to and informed by relevant institutes, also to coordinate the company’s support activities with their policies; - An innovation fund to stimulate new developments.
Another effort that turned out to be effective, was the foundation of a fund that would help local care providers with investment in their innovative efforts in development of actual care: an action that rendered a very positive renumeration of both company and brand. It is an example of a market directed action that stimulates care providers to develop into a direction of better care. In essence it is not commercial. Actually, to the contrary, when you see the needed budgets. But it signifies the opportunity to create lenient market conditions for the company’s activities when their intention is in line with the goals of health care protagonists. The company was enabled to set up such a foundation with key opinion leaders at the decision making board, without company personnel participating in this. As a result, the company’s image began to be known as innovative and cooperative to care, instead of mere commercial and ‘pushy’; - Effective market access goes beyond diverse institutes relevant to market launch.
Certainly when local protocol committees are formed to decide on preference schemes for medication, one needs to acknowledge these as access bodies too. Their related professionals will definitely not appreciate promotional actions by the part of pharma companies, but might instead welcome respective and detailed medical, research based discussions on pharma- and health economy related issues of therapy. Objective, relevant information to their work as decision makers will be appreciated as long as any suggestion of influence will be left aside. A complete new system of market access was designed for the whole affiliate organization; - Profiling, Segmentation and targeting.
A crucial and fundamental departure from the classic way of promotion was designed to facilitate selection of the right accounts as potential partners for innovative developments with the company’s medication therapies. When the company started to profile accounts to these ends, we investigated first what networks around the physicians were relevant to their appreciation of the characteristics of available medication. With an estimate of time and of degree of investment needed before return, we could already select the accounts most likely of success. Some years later, a more elaborate system of profiling, with specific data on both accounts organizational characteristics and qualities of care provided, was developed and built into an ICT system.
Using two matrices to integrate account parameters of quantitative and qualitative nature made it possible to list accounts from high to low chances of success with their respective potential. With it, more specific and reliable predictions could be made about effects of specific investments in those accounts that shared the same ambitions for patient care. Focus for the sales forces could easily be defined. Hence, particular account tailored plans could be made. One can imagine how this stimulated effective and satisfying account relations; - New skills and account management procedures and techniques were needed to the ambitions set for engagement with accounts.
To the point training into these key account management or rather Key Customer Focus skills were given to all relevant personnel, not only sales people though. Focused and tailor made account engagement, management and development plans were designed and implemented, often with approaches similar to more complex markets, like in cases of selling aircrafts. In this way account teams were able for instance to create and foster cooperation between physicians and pharmacists to increase support to patients with chronic conditions. When later on, the Dutch minister of health introduced demands regarding integrating efforts of care for chronic diseases, the company was able to profit from the already existing cooperative relations; - Flexible Design of sales teams.
Throughout the development of the approach over sales cycles, new opportunities for support to accounts emerged from closely working with them. So it appeared that physician assistants specifically assigned with tasks to oversee individual patients’ implementation of therapy, needed more insight into aspects of the disease, relevance of regular therapy control and about how to do this. In consultation with top accounts, health care consultants were added tot the account/sales teams to deliver the very support and training. Given this as an example, so, too, staffing of sales and account teams was regularly examined and got reshaped over the course of sales and marketing cycles; - Alignment of internal departments.
Being in close relation with accounts who are developing their actual care, one is enabled to early detection of emerging problems and might look for solutions to them. Direct evaluations of such calls for support are needed then for investments by brand management teams. These are typically multidisciplinary teams with representatives from all departments within the pharma company. Close cooperation between medical and marketing personnel with sales and account teams was asked for: once to the design of service solutions, secondly to investment deicsions. However, dissatisfied with the quality of their actual discussions, we began to look for methods of deliberation that would overcome hierarchical structures and other barriers to free discussion and debate, needed to find creative solutions to genuine challenges. A model for multidisciplinary design of account approach and development, was created. It functions as a tool of synchronization and alignment of the different disciplines and areas of decision making within the company. - Development of account relations in different stages.
Due to years of building promotion routines of detailing, pharma is not familiar with development of sustainable relations of cooperation and partnership with accounts. Promotional relations and incidental service work in project format, is quite a different thing than building partnership to work together to co-create new formats and routines for care. Building relations needs trusted and reliable partners. Intensive collaboration will not emerge instantly: it needs confirmation over time.
That’s why customer facing personnel needs to know what the subsequent stages in development of partnership are, and how to work to build trust and reliability. We developed a model for that, also to alert professionals to conditions of interaction and of communication and hence of desired behavior in subsequent stages. The model that we developed defines the subsequent development stages and signifies crucial elements of collaboration that indicates an upgrade to a next level of working together.


Implementation
We became quickly aware that implementation of a new market approach is not a process of installment but a process of continuous change and development. That makes it more difficult to sustain and lead the desired changes. But beware, the process is not a matter of checklists of activities that need to be ticked subsequently. The desired changes may demand change of attitude, new skills, change of internal procedures, installment of new functions, and the like. The more the chosen strategy is further away from classic, standardized detailing, the more structural the changes will be. So it is wise to assure step by step development to create a cascade of subsequent steps over cycles of implementation.
In a commercial perspective it would mean to “pick the lowest hanging fruits” first. Next further development needs to create focus to effective actions and addded value to selected accounts. If so, more information about new variables will be needed. The better the profiling of conditions is done, the more effective early development steps can be defined, also in terms of costs and energy.
Change and development of the market approach cannot be done without the right understanding and abilities of people to perform it. Certainly not when understanding of new areas of concern are at stake, like physician patient interaction and communication.
Demanded new competencies are not to be expected overnight, nor to be communicated and acquired by technology only. It might even imply selection of people with the right attitudes and capabilities. A developmental approach, that allows for genuine learning and development of the part of pharma’s personnel, and management too, will allow for growth or selection of personnel.
Hence, applying this commercial model to pharma’s market approach is about change and decision making, about focus and added value. Added value to care upon the medication to use in therapy. As the trends in health care point to development of personal care and of concordance between providers and patients, we will see more parties to care cooperatively in the process. Pharma has to decide on whether and how to develop its position to this development. So in essence, the application is about change and innovation to the organization, not just of implementing yet another new program. It will be a roadmap with a moving end. One must decide in the context of system developments of care and regulations. So it will be best to learn as an organization how change can be made permanent to it. There are several ways to do so. Every market and affiliate will have its own best and optimal way for effectiveness and efficiency. Implementing global strategies are about differentiation.
To conclude, a reflection to share
You might have already detected that the model has been used by us to guide a pharma company to close cooperation with accounts to help them improve their patient care. So, that is more to the strategic end of adding value to escape the commodity trap. As indicated, it proved to be the right strategic choice.
Preferences or even necessity for the opposite might also be realistic: it will lead however to more focus for decision makers to buying of drugs in hospitals, health insurance, governmental, HMO-like or wholesale organizations. These will decide on criteria of costs, not so much on care. It might need care providers and patients organizations to speak out for their interests. 
As indicated too, cost effectiveness and USP’s in supply chain perspective might help. Even then, examples of direct supply to patients demonstrate pharma’s relationship with patient care: in tailor made patient packaging and reminders of medication. It will take time for decision makers to acknowledge that the ‘cheapest’ options will turn out to be expensive in the long run.
The more substantial roadmap for development will be grounded in health and pharma related economic considerations about medication, regarding prescription and therapy routines with it. There’s no alternative I think, to integrative perspectives to care. This model will help pharma to grow as a respected partner to care.
References
¹Regarding literature on Pharma’s new business model, commercial model, sales model, etc. a grand list of publications is too long to present here. Drop me a line to have it sent to you, if you so wish;
²See for an example of the discussion about the effectiveness of standard detailing here;
³ Bryan Lawson, How designers think, the design process demystified, Oxford 2005.
Also: Donald, A, Schön, The reflective practitioner, how professionals think in action. Aldershot, England 1998.